Triple monitoring a multimodal safety approach for PNBs
Peripheral nerve blockade (PNB) is a widely practiced technique used to provide anesthesia during surgical procedures (e.g. surgery of the arm) and invasive pain control (e.g. rib fracture) during peri-operative process. Continuous improvements of clinical training and techniques in combination with smart products are the main drivers to reduce side effects and increase safety.
Nerve injury and resulting postoperative neurologic dysfunction (PONS) is a feared complication of peripheral nerve blockade. Estimates of its incidence vary from as little as 0.18% to as much as 16%, depending on the site the block was performed on and the technique.1
The majority of neurologic symptoms following nerve blockade are transient and last a few hours to days, but some are permanent and can result in profound disability, depending on the level of nerve trauma caused. 2-4
Escalation of Nerve Trauma5
Even if the main focus is on patients suffering from nerve trauma emotionally and from prolonged rehabilitation, there are other costs associated with these adverse events. These include the cost of prolonged length of stay and/or neurologic testing, the emotional and financial strain of missed work, and the negative impact on the patient’s day-to-day quality of life. Many patients with long-term nerve injuries following a nerve block eventually seek compensation through the legal system, incurring further expenses for both the patient and for the caregivers and facility.

To prevent the occurrence of the described neurological complications, the interpretation of the various information available when performing PNBs are of key importance. Evidence has emerged that the use of objective information from complementary monitoring modalities help to prevent neurological complications to guide more informed decisions for needle tip placement and local anesthetic injection. Ultrasound, objective injection pressure monitoring and nerve stimulation are synergistic and additive, offering the clinicians with complementary information to get the broadest picture possible. The sequence as recommended by NYSORA when performing nerve blocks using the multiple monitors is outlined in the flowchart below.
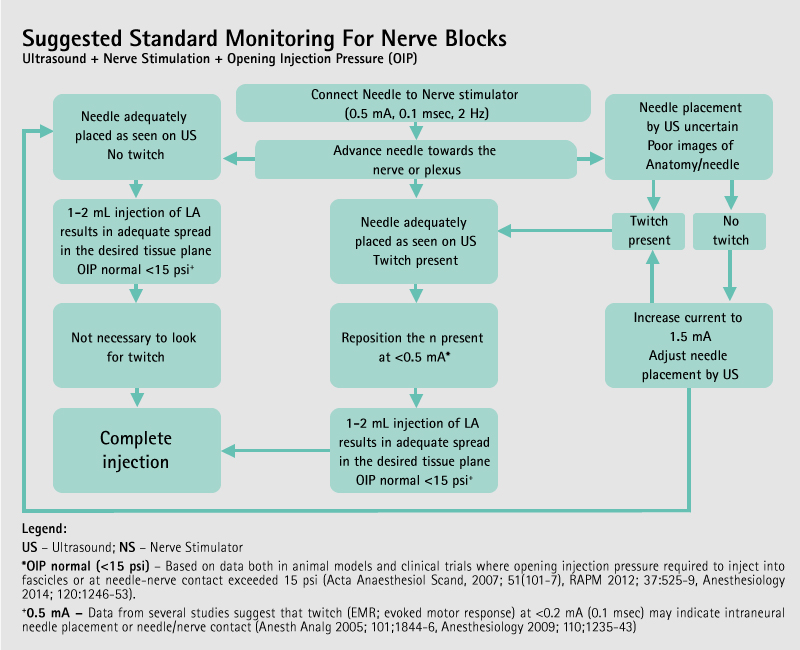
During the nerve block procedure the values displayed on the three individual monitors can be documented with clear and objective values that bring evidence in the routine of performing peripheral nerve blocks.
References
- Sites BD, Taenzer AH, Herrick MD, Gilloon C, Antonakakis J, Richins J, Beach ML: Incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms associated with 12,668 ultrasound-guided nerve blocks: an analysis from a prospective clinical registry. Reg Anesth Pain Med 2012; 37:478–82
- Liu SS, YaDeau JT, Shaw PM, Wilfred S, Shetty T, Gordon M: Incidence of unintentional intraneural injection and postoperative neurological complications with ultrasound-guided interscalene and supraclavicular nerve blocks. Anaesthesia 2011; 66:168–74
- Bilbao Ares A, Sabaté A, Porteiro L, Ibáñez B, Koo M, Pi A: [Neurological complications associated with ultrasound-guided interscalene and supraclavicular block in elective surgery of the shoulder and arm. Prospective observational study in a university hospital.]. Rev Esp Anestesiol Reanim 2013doi:10.1016/j.redar.2013.02.016
- Widmer B, Lustig S, Scholes CJ, Molloy A, Leo SPM, Coolican MRJ, Parker DA: Incidence and severity of complications due to femoral nerve blocks performed for knee surgery. Knee 2013; 20:181–5
- Steinfeldt T, Needle trauma and current monitoring, 2015, internal data on file